Will Severs Disease Call For Surgical Treatments?
Overview
When recurring heel pain occurs in children, it is usually due to Sever's Disease, while adult heel pain is usually due to heel spurs, plantar fasciitis, or retrocalcaneal bursitis (Haglund's Deformity). Calcaneus is the anatomical name of the heel bone. Sever's Disease or Calcaneal Apophysitis is an inflammation of the growth plate located at the posterior aspect (back) of the heel.
Causes
Severs disease is often associated with a rapid growth spurt. As the bones get longer, the muscles and tendons become tighter as they cannot keep up with the bone growth. The point at which the achilles tendon attaches to the heel becomes inflamed and the bone starts to crumble (a lot like osgood schlatters disease of the knee). Tight calf muscles may contribute as the range of motion at the ankle is reduced resulting in more strain on the achilles tendon. Sever's disease is the second most common injury of this type which is known as an apophysitis.
Symptoms
Sharp pain will be present in the affected heel (or both heels), especially while running or walking. Pain can be heightened following activity. The area will be tender to the touch and usually becomes inflamed or reddened. It may also be painful to press on the heel with a finger from the back or to squeeze the sides together; the latter is particularly common. You might notice stiffness in some of the surrounding muscles, making regular movements more difficult to achieve. This and the pain can manifest physically in abnormal practices like tiptoeing or limping. In some cases a lump can be detected on the back of the heel, though it may be so small as to defy detection.
Diagnosis
You may have pain when your doctor squeezes your heel bone. You may have pain when asked to stand or walk on your toes or on your heels. You may have pain in your heel when your doctor stretches your calf muscles. Your doctor may order x-rays of the injured foot to show an active growth plate.
Non Surgical Treatment
Sever?s disease is a self-limiting problem, because as your child grows the growth plate will eventually fuse with the main body of the heel bone. This happens at about 14 -15 years of age. Once foot growth is complete and the growth plate has fused, the symptoms will resolve. In the meantime, treatment by your Podiatrist will help your child return to normal sporting activities without heel pain slowing him/her down.
When recurring heel pain occurs in children, it is usually due to Sever's Disease, while adult heel pain is usually due to heel spurs, plantar fasciitis, or retrocalcaneal bursitis (Haglund's Deformity). Calcaneus is the anatomical name of the heel bone. Sever's Disease or Calcaneal Apophysitis is an inflammation of the growth plate located at the posterior aspect (back) of the heel.
Causes
Severs disease is often associated with a rapid growth spurt. As the bones get longer, the muscles and tendons become tighter as they cannot keep up with the bone growth. The point at which the achilles tendon attaches to the heel becomes inflamed and the bone starts to crumble (a lot like osgood schlatters disease of the knee). Tight calf muscles may contribute as the range of motion at the ankle is reduced resulting in more strain on the achilles tendon. Sever's disease is the second most common injury of this type which is known as an apophysitis.
Symptoms
Sharp pain will be present in the affected heel (or both heels), especially while running or walking. Pain can be heightened following activity. The area will be tender to the touch and usually becomes inflamed or reddened. It may also be painful to press on the heel with a finger from the back or to squeeze the sides together; the latter is particularly common. You might notice stiffness in some of the surrounding muscles, making regular movements more difficult to achieve. This and the pain can manifest physically in abnormal practices like tiptoeing or limping. In some cases a lump can be detected on the back of the heel, though it may be so small as to defy detection.
Diagnosis
You may have pain when your doctor squeezes your heel bone. You may have pain when asked to stand or walk on your toes or on your heels. You may have pain in your heel when your doctor stretches your calf muscles. Your doctor may order x-rays of the injured foot to show an active growth plate.
Non Surgical Treatment
Sever?s disease is a self-limiting problem, because as your child grows the growth plate will eventually fuse with the main body of the heel bone. This happens at about 14 -15 years of age. Once foot growth is complete and the growth plate has fused, the symptoms will resolve. In the meantime, treatment by your Podiatrist will help your child return to normal sporting activities without heel pain slowing him/her down.
Causes Symptoms And Therapy For An Achilles Tendon Rupture
Overview
 A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
A rupture of the Achilles tendon means that there has been either a complete, or partial, tear of the tendon which connects the calf muscles to the heel bone. Usually this occurs just above insertion on the heel bone, although it can happen anywhere along the course of the tendon.
Causes
The Achilles tendon can grow weak and thin with age and lack of use. Then it becomes prone to injury or rupture. Achilles tendon rupture is more common in those with preexisting tendinitis of the Achilles tendon. Certain illnesses (such as arthritis and diabetes) and medications (such as corticosteroids and some antibiotics, including quinolones such as levofloxacin [Levaquin] and ciprofloxacin [Cipro]) can also increase the risk of rupture. Rupture most commonly occurs in the middle-aged male athlete (the weekend warrior who is engaging in a pickup game of basketball, for example). Injury often occurs during recreational sports that require bursts of jumping, pivoting, and running. Most often these are tennis, racquetball, basketball, and badminton. The injury can happen in the following situations. You make a forceful push-off with your foot while your knee is straightened by the powerful thigh muscles. One example might be starting a foot race or jumping. You suddenly trip or stumble, and your foot is thrust in front to break a fall, forcefully overstretching the tendon. You fall from a significant height or abruptly step into a hole or off of a curb.
Symptoms
Patients often describe a feeling of being kicked or hit with a baseball bat in the back of the heel during athletic activity. They are unable to continue the activity and have an extreme loss of strength with the inability to effectively walk. On physical examination there is often a defect that can be felt in the tendon just above the heel. A diagnosis of an Achilles tendon rupture is commonly made on physical exam. An MRI may be ordered to confirm the suspicion of a tear or to determine the extent of the tear.
Diagnosis
Your caregiver will ask what you were doing at the time of your injury. You may need any of the following. A calf-squeeze test is used to check for movement. You will lie on your stomach on a table or bed with your feet hanging over the edge. Your caregiver will squeeze the lower part of each calf. If your foot or ankle do not move, the tendon is torn. An x-ray will show swelling or any broken bones. An ultrasound uses sound waves to show pictures of your tendon on a monitor. An ultrasound may show a tear in the tendon. An MRI takes pictures of your tendon to show damage. You may be given dye to help the tendon show up better. Tell the caregiver if you have ever had an allergic reaction to contrast dye. Do not enter the MRI room with anything metal. Metal can cause serious injury. Tell the caregiver if you have any metal in or on your body.
Non Surgical Treatment
You may need to wear a plaster cast, brace or boot on your lower leg for six to eight weeks to help the tendon heal. During this time, your doctor will change the cast a number of times to make sure your tendon heals in the right way. If your tendon is partially ruptured, your doctor will probably advise you to have this treatment instead of surgery. It?s also suitable for people who aren't very physically active. However, there is a greater risk that your tendon will rupture again, compared with surgery. Your doctor will advise you which treatment is best for you. 
Surgical Treatment
Surgery to repair an Achilles tendon rupture is performed under a spinal or general anaesthetic. During surgery the surgeon makes an incision in the skin over the ruptured portion of the tendon. The tendon ends are located and joined together with strong sutures (stitches), allowing the tendon to closely approximate its previous length. The skin is then closed with sutures and the foot is immobilised in a cast or splint, again in the toes-pointed position. Seven to ten days after surgery the cast or splint is removed in order for the sutures in the skin to be removed. Another cast or splint will be applied and will stay in place a further 5 - 7 weeks.
Leg Length Discrepancy Shoe Lifts
Overview
Leg length discrepancy (LLD) affects about 70% of the general population, and can be either structural - when the difference occurs in bone structures - or functional, because of mechanical changes at the lower limbs. The discrepancy can be also classified by its magnitude into mild, intermediate, or severe. Mild LLD has been particularly associated with stress fracture, low back pain and osteoarthritis, and when the discrepancy occurs in subjects whose mechanical loads are increased by their professional, daily or recreational activities, these orthopaedic changes may appear early and severely. The aim of this study was to analyze and compare ground reaction force (GRF) during gait in runners with and without mild LLD. Results showed that subjects with mild LLD of 0.5 to 2.0 cm presented higher values of minimum vertical GRF (0.57 ? 0.07 BW) at the shorter limb compared to the longer limb (0.56 ? 0.08 BW) Therefore, subjects with mild LLD adopt compensatory mechanisms that cause additional overloads to the musculoskeletal system in order to promote a symmetrical gait pattern as showed by the values of absolute symmetric index of vertical and horizontal GRF variables.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
Children whose limbs vary in length often experience difficulty using their arms or legs. They might have difficulty walking or using both arms to engage in everyday activities.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
In some circumstances, the physician will recommend a non-surgical form of treatment. Non-surgical treatments include orthotics and prosthetics. Orthotics are a special type of lift placed in or on a shoe that can be used in the treatment of leg length discrepancies between two and six centimeters. In pediatric patients who have large discrepancies and are not good candidates for other treatment forms, prosthetics can be helpful.

Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Leg length discrepancy (LLD) affects about 70% of the general population, and can be either structural - when the difference occurs in bone structures - or functional, because of mechanical changes at the lower limbs. The discrepancy can be also classified by its magnitude into mild, intermediate, or severe. Mild LLD has been particularly associated with stress fracture, low back pain and osteoarthritis, and when the discrepancy occurs in subjects whose mechanical loads are increased by their professional, daily or recreational activities, these orthopaedic changes may appear early and severely. The aim of this study was to analyze and compare ground reaction force (GRF) during gait in runners with and without mild LLD. Results showed that subjects with mild LLD of 0.5 to 2.0 cm presented higher values of minimum vertical GRF (0.57 ? 0.07 BW) at the shorter limb compared to the longer limb (0.56 ? 0.08 BW) Therefore, subjects with mild LLD adopt compensatory mechanisms that cause additional overloads to the musculoskeletal system in order to promote a symmetrical gait pattern as showed by the values of absolute symmetric index of vertical and horizontal GRF variables.
Causes
Leg length discrepancies can be caused by poor alignment of the pelvis or simply because one leg is structurally longer than the other. Regardless of the reason, your body wants to be symmetrical and will do its best to compensate for the length difference. The greater the leg length difference, the earlier the symptoms will present themselves to the patient. Specific diagnoses that coincide with leg length discrepancy include: scoliosis, lumbar herniated discs, sacroiliitis, pelvic obiliquity, greater trochanteric bursitis, hip arthritis, piriformis syndrome, patellofemoral syndrome and foot pronation. Other potential causes could be due to an injury (such as a fracture), bone disease, bone tumors, congenital problems (present at birth) or from a neuromuscular problem.
Symptoms
Children whose limbs vary in length often experience difficulty using their arms or legs. They might have difficulty walking or using both arms to engage in everyday activities.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
In some circumstances, the physician will recommend a non-surgical form of treatment. Non-surgical treatments include orthotics and prosthetics. Orthotics are a special type of lift placed in or on a shoe that can be used in the treatment of leg length discrepancies between two and six centimeters. In pediatric patients who have large discrepancies and are not good candidates for other treatment forms, prosthetics can be helpful.
Surgical Treatment
In growing children, legs can be made equal or nearly equal in length with a relatively simple surgical procedure. This procedure slows down the growth of the longer leg at one or two growth sites. Your physician can tell you how much equalization can be gained by this procedure. The procedure is performed under X-ray control through very small incisions in the knee area. This procedure will not cause an immediate correction in length. Instead, the limb length discrepancy will gradually decrease as the opposite extremity continues to grow and "catch up." Timing of the procedure is critical. The goal is to reach equal leg length by the time growth normally ends. This is usually in the mid-to-late teenage years. Disadvantages of this option include the possibility of slight over-correction or under-correction of the limb length discrepancy. In addition, the patient's adult height will be less than if the shorter leg had been lengthened. Correction of significant limb length discrepancy by this method may make a patient's body look slightly disproportionate because of the shorter leg. In some cases the longer leg can be shortened, but a major shortening may weaken the muscles of the leg. In the thighbone (femur), a maximum of 3 inches can be shortened. In the shinbone, a maximum of 2 inches can be shortened.
Flexible Flat Feet In Adults
Overview
When we have foot pain, it isn?t always easy to pinpoint the source because we can?t visualize the structure of all the bones, muscles, and tendons on the inside. The posterior tibial tendon plays an important supportive role within the structure of the foot. It attaches to your calf muscle and then comes down along the inside of your ankle, connecting to the bones inside your foot at the other side. This tendon?s main function is to hold up your arch and support your foot during each and every movement. Every step, run, walk, or jump is made possible with the support from this crucial tendon. While it is designed to perform such an important role, it is vulnerable to stress and injury. A tear during a traumatic injury or stress from overuse can injure the tissues within the tendon. This kind of injury is referred to as posterior tibial tendon dysfunction (PTTD). A really hard fall during a sports game or exposure to a repetitive motion, such as the impact on feet during soccer, tennis, football or basketball, can cause an injury. Flat foot and flat feet in adults can exacerbate this condition. The tendon can experience small tears and become inflamed. If the inflammation is allowed to continue and worsen over time, it will weaken further and could rupture completely. 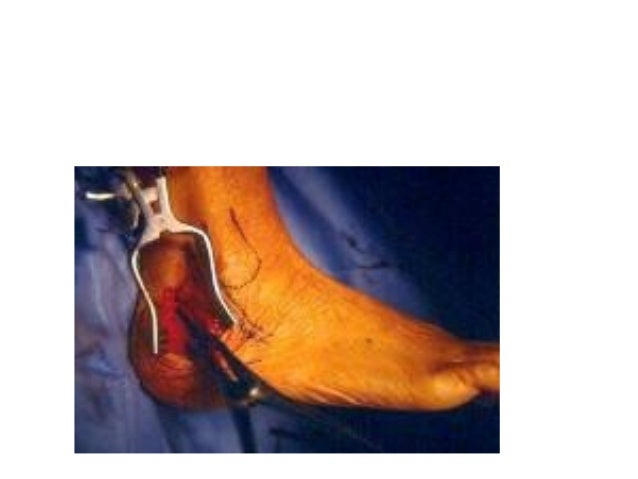
Causes
As discussed above, many different problems can create a painful flatfoot. Damage to the posterior tibial tendon is the most common cause of AAFD. The posterior tibial tendon is one of the most important tendons of the leg. It starts at a muscle in the calf, travels down the inside of the lower leg and attaches to the bones on the inside of the foot. The main function of this tendon is to support the arch of your foot when you walk. If the tendon becomes inflamed or torn, the arch will slowly collapse. Women and people over 40 are more likely to develop problems with the posterior tibial tendon. Other risk factors include obesity, diabetes, and hypertension. Having flat feet since childhood increases the risk of developing a tear in the posterior tibial tendon. In addition, people who are involved in high impact sports, such as basketball, tennis, or soccer, may have tears of the tendon from repetitive use. Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the tendons or ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. Injuries to tendons of the foot can occur either in one instance (traumatically) or with repeated use over time (overuse injury). Regardless of the cause, if tendon function is altered, the forces that are transmitted across joints in the foot are changed and this can lead to increased stress on joint cartilage and ligaments. In addition to tendon and ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with nerve problems that limits normal feeling in the feet, can have collapse of the arch or of the entire foot. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem.
Symptoms
Pain and swelling around the inside aspect of the ankle initially. Later, the arch of the foot may fall (foot becomes flat), this change leads to walking to become difficult and painful, as well as standing for long periods. As the flat foot becomes established, pain may progress to the outer part of the ankle. Eventually, arthritis may develop.
Diagnosis
The adult acquired flatfoot, secondary to posterior tibial tendon dysfunction, is diagnosed in a number of ways with no single test proven to be totally reliable. The most accurate diagnosis is made by a skilled clinician utilizing observation and hands on evaluation of the foot and ankle. Observation of the foot in a walking examination is most reliable. The affected foot appears more pronated and deformed compared to the unaffected foot. Muscle testing will show a strength deficit. An easy test to perform in the office is the single foot raise. A patient is asked to step with full body weight on the symptomatic foot, keeping the unaffected foot off the ground. The patient is then instructed to "raise up on the tip toes" of the affected foot. If the posterior tibial tendon has been attenuated or ruptured, the patient will be unable to lift the heel off the floor and rise onto the toes. In less severe cases, the patient will be able to rise on the toes, but the heel will not be noted to invert as it normally does when we rise onto the toes. X-rays can be helpful but are not diagnostic of the adult acquired flatfoot. Both feet - the symptomatic and asymptomatic - will demonstrate a flatfoot deformity on x-ray. Careful observation may show a greater severity of deformity on the affected side.
Non surgical Treatment
Patients can be treated non-surgically with in-shoe devices and braces to hold their feet in the correct position. This can reduce pain and damage and assist with walking. Physical therapy is also given to improve muscle strength and help prevent injury to the foot. Surgery can be performed if the patient doesn?t find any relief. 
Surgical Treatment
Good to excellent results for more than 80% of patients have been reported at five years' follow up for the surgical interventions recommended below. However, the postoperative recovery is a lengthy process, and most surgical procedures require patients to wear a plaster cast for two to three months. Although many patients report that their function is well improved by six months, in our experience a year is required to recover truly and gain full functional improvement after the surgery. Clearly, some patients are not candidates for such major reconstructive surgery.